
Your special needs intake process probably breaks down the same way every time. Parents fill out standard enrollment forms, maybe check a box about "developmental concerns," and three weeks later a teacher pulls you aside because Maya hasn't spoken once, Tommy has daily meltdowns during transitions, or Sarah needs physical support that was never disclosed.
The gap between what families share during enrollment and what their child actually needs creates a real operational mess. Teachers scramble to modify activities on the fly. Parents get frustrated when their child struggles. Other families start complaining about disruptions. And you're stuck retrofitting support systems mid-enrollment while managing behavior incidents that could've been prevented with better information upfront.
Most centers handle special needs reactively—waiting until problems surface, then scrambling. Centers that build proactive intake and documentation systems catch needs early, staff appropriately, and avoid most of the downstream chaos.
The intake gap that creates cascading problems
Standard enrollment forms fail special needs families because they're built for neurotypical children. A checkbox asking "does your child have any developmental concerns?" gets you almost nothing. Parents may not recognize delays, feel uncomfortable disclosing, or genuinely assume you'll figure it out once their child starts.
A parent enrolls their 3-year-old who "just needs a little extra help with transitions." Two weeks in, you discover the child has sensory processing issues, requires a weighted vest, needs visual schedules, and has never been in group care. Your lead teacher is now spending 40% of her time managing one child while 11 others wait.
The breakdown happens in layers. Your enrollment coordinator doesn't know what questions to ask beyond basic medical forms. Parents who've never navigated special needs support don't know what information matters. Teachers inherit situations they're not trained or staffed to handle. And by the time everyone realizes the mismatch, the family has paid tuition, the child has started bonding with peers, and you're either scrambling to accommodate or having a very uncomfortable conversation about fit.
Centers lose families in both directions. Special needs families leave when their child's needs aren't met. Other families leave when one child's unmanaged behaviors dominate classroom attention. Teachers burn out trying to bridge support gaps without proper resources. It compounds fast.
Building an intake process that actually captures needs
Effective special needs intake starts before enrollment with a two-stage process. First, a preliminary screening call that normalizes discussing developmental variations. Then an in-person observation session where trained staff can actually see how the child functions in a group setting.
Simplify your childcare center’s daily operations.
Totsyly helps you manage enrollments, staff, and communications efficiently so you can focus on care.
- Streamlined enrollment & waitlist management
- Automated billing & payment tracking
- Staff scheduling & attendance monitoring
No credit card required
The screening call shifts away from "Does your child have special needs?" toward specific behavioral questions:
-
How does your child handle unexpected changes to routine?
-
What helps calm them when upset?
-
Do loud noises, bright lights, or certain textures cause distress?
-
How do they communicate when hungry, tired, or needing the bathroom?
-
What does a typical meltdown look like, and how long does recovery take?
Parents answer these easily because they're about daily life, not diagnostic labels. You learn that Emma needs advance warning before transitions, Marcus covers his ears during music time, and Lily uses an AAC device—information that never would've appeared on a standard form.
The observation session comes next. Instead of a standard enrollment tour, the child participates in a 45-minute sample day with current students. A trained observer documents how they handle circle time, peer interactions, transitions, and sensory experiences. You see whether they can follow two-step directions, share materials, or stay regulated during typical activities.
Schedule the observation during a typical activity window (snack or circle) so you see transitions and routine-based triggers.
This two-stage process catches the majority of support needs before enrollment. More importantly, it opens an honest conversation with families about what accommodations you can realistically provide versus what might require additional resources or a different setting.
The individualized plan that prevents daily firefights
Once you identify support needs, the standard practice at most centers is adding notes to the child's file and hoping teachers remember. This fails almost immediately. The lead teacher knows Emma needs transition warnings, but the afternoon assistant doesn't. The music teacher wasn't told about Marcus's sound sensitivity. Lily's AAC device instructions never made it to the substitute folder.
Centers that handle this well create living support documents that travel with the child throughout their day. Not lengthy IEP-style documents that no one reads—practical one-page plans that any staff member can pick up and use in under a minute.
The plan captures five operational elements:
Triggers and preventions: What causes dysregulation and how to avoid it. "Sudden loud noises cause covering ears and crying. Give warning before fire drills. Offer noise-reducing headphones during music."
Regulation strategies: Specific techniques that work for this child. "Deep pressure helps during meltdowns. Apply firm shoulder squeezes. Offer weighted lap pad during circle time."
Communication methods: How the child expresses needs and how to respond. "Points to picture cards for bathroom and water. Uses 'all done' sign when overwhelmed. Watch for hand-flapping as early frustration signal."
Transition supports: The exact routine for difficult transitions. "Five-minute warning with timer. Show visual of next activity. Allow to carry comfort object. Count down from 10 before moving."
Parent coordination: What needs to be communicated daily. "Document any hitting incidents for behavior tracking. Note food consumed for feeding therapy. Send photo of completed art for home reinforcement."
These plans live in three places: laminated in the classroom, digital in your management system, and abbreviated on the daily roster. Any adult who interacts with the child—regular teacher, afternoon floater, or sub—has immediate access to what actually works.
Staffing models that don't blow up ratios
The standard mistake with special needs children is assuming you can maintain typical ratios with strategic placement. Put the high-needs kids together so one teacher can specialize. Spread them across rooms to "balance" the load. Float an extra aide between classrooms as needed.
These models break down fast under real operational pressure. The specialized teacher calls out sick and no one else knows the plans. The spread-out approach means four teachers need specialized training. The floating aide is inevitably in the wrong room when a situation escalates.
Centers that do this well use adaptive staffing that builds in redundancy:
The overlay model: Instead of dedicated one-on-one aides, you add an additional teacher for every 3-4 children with documented support needs, regardless of room assignment. This teacher works across classrooms but carries primary responsibility for those specific children. When she's out, another overlay teacher already knows these children from regular rotation.
The pod structure: Classrooms are paired, with two teachers who cross-train on all special needs children in both rooms. Room A's lead knows Room B's support plans and vice versa. Coverage during breaks comes from the paired room's teacher who already knows the kids.
The specialist rotation: Instead of classroom-assigned staff, you have two or three special education-trained floaters who rotate through all rooms on a set schedule. Every special needs child gets dedicated support time daily, without depending on any single staff member being present.
A center with 6 special needs children across 4 classrooms might combine approaches: overlay teachers for the 3 highest-needs children, pod structure for consistent coverage, and specialist rotation for weekly skill-building sessions. The point is redundancy—no child's support should depend entirely on one person showing up.
This costs more than standard ratios, somewhere in the range of $400–600 per special needs child monthly in additional staffing. But that's far less than the cost of losing families, managing escalating behavior incidents, or cycling through burned-out teachers.
Documentation workflows that keep everyone aligned
The typical documentation pattern with special needs children is reactive crisis recording. An incident happens, someone writes it up, it goes in a file. Parents hear about problems after they've already escalated. Specialists get reports weeks after patterns emerged. Staff figure out support strategies through trial and error.
Proactive documentation changes the whole dynamic. You're tracking patterns before they become problems, sharing what works in real time, and building institutional knowledge that actually improves care.
The workflow runs three parallel tracks:
-
Daily communication logs capture routine information that builds patterns over time. Not lengthy narratives—quick structured data. Arrival mood (scale 1–5), transition success, peer interactions, regulation incidents (time, trigger, duration, intervention used). Takes under two minutes per child but reveals patterns that are completely invisible in day-to-day observations.
-
Strategy sharing happens through a simple what-worked system. When any staff member finds an effective approach, they document it immediately in a shared space. "Marcus stayed calm during music when given a rice-filled stress ball." "Lily initiated peer play when we used her favorite dinosaur book as a conversation starter." These micro-discoveries reach all staff within hours, not weeks.
-
Specialist coordination runs through a central communication hub instead of scattered emails and paper notes. The speech therapist sees yesterday's communication attempts. The OT knows which sensory strategies the teacher tried. The behavioral specialist tracks incident patterns across settings. Parents access daily updates and can add home observations that inform the next day's approach.
One center implemented this for their 8 special needs students across 3 classrooms. Within six weeks, behavior incidents had dropped by roughly 60%—not because the children had suddenly improved, but because staff could anticipate and prevent escalations using documented patterns and proven strategies.
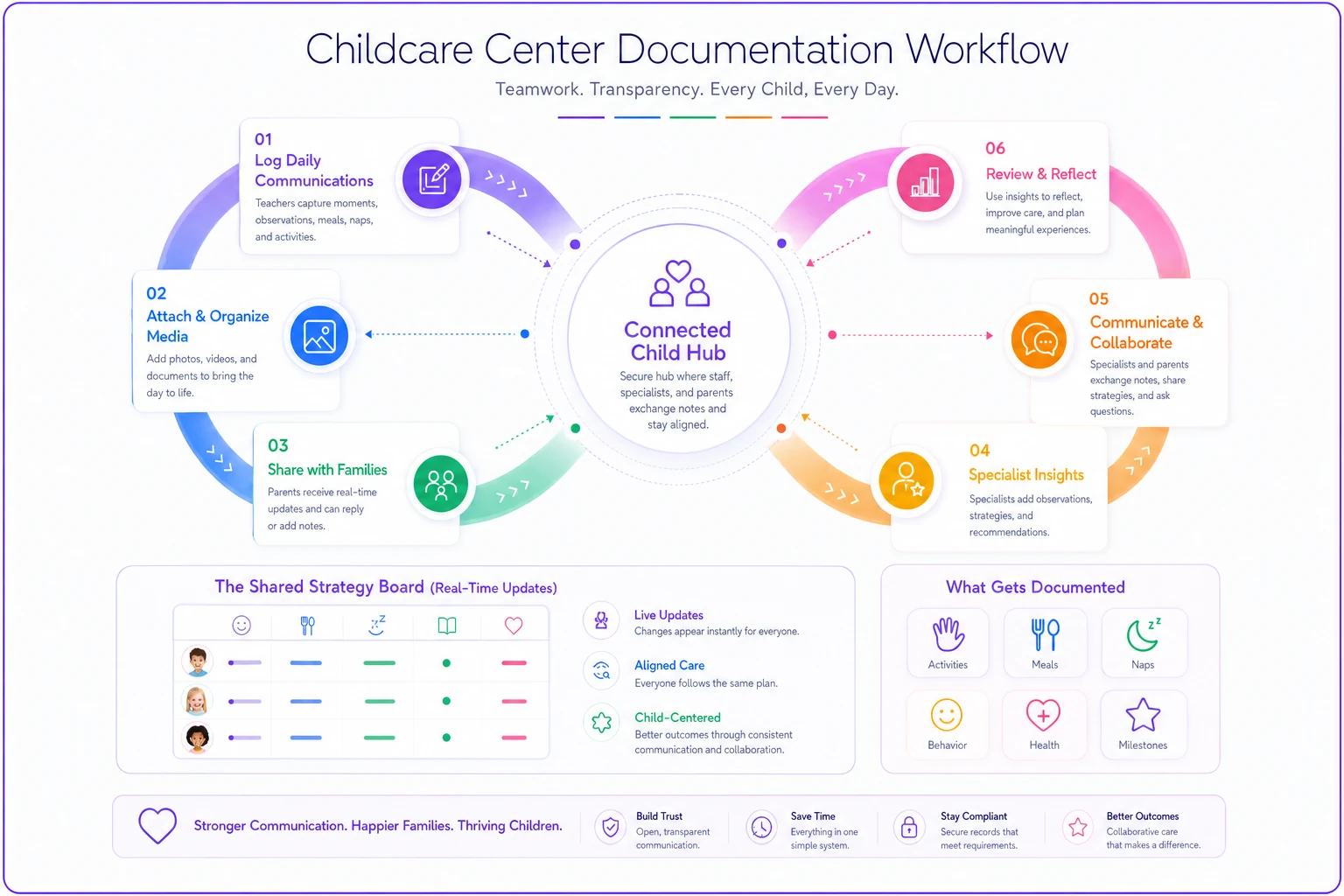
This visualization shows how quick logs, immediate strategy sharing, and a central specialist hub keep everyone informed and able to act before incidents escalate.
The family partnership that prevents placement failures
Most special needs placements fail because of misaligned expectations, not actual incompatibility. Families expect more support than you can provide. You expect strategies that work at home to translate directly to group care. Both sides assume the other understands needs that were never explicitly discussed.
Successful partnerships start with transparency during intake. Not promises—actual practice. "We can provide visual schedules and transition warnings. We cannot provide one-on-one assistance during meals. We can offer quiet spaces for regulation. We cannot implement full ABA programs."
Then you build structured check-ins that catch problems before they become deal-breakers. Not annual IEP-style meetings—short weekly conversations at pickup, maybe 10 minutes:
-
What's working well this week?
-
What's been challenging?
-
What should we try differently?
-
What are you seeing at home?
-
What do you need from us?
These conversations get documented in your communication platform, with patterns reviewed monthly by leadership. You catch when a family needs more than you can realistically provide before frustration builds into a crisis.
The specialist coordination piece requires its own workflow. Instead of hoping families share therapy reports or remember to mention medication changes, build information exchange into enrollment agreements. Families sign releases allowing direct communication with their child's therapy team. Specialists get monthly updates on center observations. You get copies of evaluation reports and therapy goals.
A practical example: Tommy's occupational therapist recommends a sensory diet with heavy work activities every two hours. Instead of expecting teachers to interpret a vague therapy report, you translate that into specific classroom activities—carrying the snack basket, pushing chairs after lunch, pulling the wagon during outdoor play. The therapist confirms these meet the sensory diet requirements. Teachers have concrete tasks instead of abstract goals.
The actual ROI of getting this right
Centers resist building comprehensive special needs systems because they see only costs: additional staffing, training time, documentation burden. But the financial impact of not having these systems is consistently worse.
| Scenario | Without Systems | With Systems |
|---|---|---|
| Needs identified | Week 3 (reactive) | Before enrollment |
| Staffing adjustment | Emergency, mid-enrollment | Planned, budgeted |
| Family retention | Often lost within 2 months | Multi-year enrollment |
| Incident volume | High, escalating | Reduced significantly |
| Additional cost | Lost tuition + admin time | ~$400–600/month |
A typical scenario without proper support: You enroll a child with undisclosed sensory needs. Three weeks in, daily meltdowns during transitions. Other parents start complaining. You lose two families who cite "classroom management issues." The child's family leaves after two months, frustrated. You spend 40-plus hours managing the situation, documenting incidents, and meeting with upset parents. Total impact: several thousand dollars in lost tuition, significant administrative time, and reputation damage in local parent groups.
With proper systems in place, the intake process identifies sensory needs before enrollment. You staff appropriately and create support plans. Transitions include sensory breaks and advance warnings. Meltdowns drop dramatically. The family stays enrolled for years and refers other special needs families. Additional staffing costs around $500 monthly, but you retain tuition that would otherwise be gone. The math works out fairly quickly.
The less visible returns compound over time. Teachers stay longer when they feel supported managing challenging behaviors. Your reputation as an inclusive center attracts families willing to pay for quality. Your staff builds expertise that makes your center genuinely hard to replace for enrolled families.
Building from where you are
Most centers can't implement comprehensive special needs systems overnight, and trying to do it all at once usually leads to doing none of it well. A reasonable build sequence looks like this:
-
Fix your intake first—screening calls and observation sessions catch the majority of undisclosed needs before enrollment begins
-
Build one-page support plans for each child with identified needs and put them everywhere staff can access them
-
Add daily structured documentation, even basic mood and incident tracking
-
Implement weekly family check-ins and document what comes out of them
-
Build specialist coordination into enrollment agreements so information flows automatically
The documentation piece is where AI-powered operational software makes a real difference. Manual tracking across paper forms, communication logs, and incident reports becomes unmanageable as enrollment grows. The right platform can surface behavioral patterns you'd otherwise miss across scattered notes, flag when a child's profile shifts over time, and route relevant updates to the right staff and specialists automatically. Instead of teachers spending 20–30 minutes on documentation at end of day, structured digital inputs take a few minutes—and the system handles distribution and analysis.
Start before you think you're ready. Every center believes they need more training, more resources, more specialist partnerships before they can accept special needs children. The real capability gets built by doing it, not by preparing indefinitely.
The competence cascade effect
Something worth paying attention to: centers that build strong special needs support systems tend to get better at supporting all children, not just those with documented needs. The teacher who learns to provide transition warnings for Marcus starts doing it for everyone. Visual schedules created for Emma help the whole class understand daily routines. Regulation strategies developed for Lily become classroom-wide calm-down techniques.
Staff develop observational skills that catch struggling children earlier. Documentation systems reveal patterns in typical development too. Communication with families becomes more substantive across the board. The infrastructure you build for your highest-needs children raises the baseline for everyone.
This changes your center's reputation in a specific way. You become known not just as "inclusive" but as genuinely attentive to individual children. Families choose you not because you're convenient or affordable but because you actually see their child. In a market where most centers compete on price and location, that differentiation drives enrollment and retention in ways that marketing rarely does.
Start with intake, build support plans that travel, staff for redundancy not just ratios, document proactively, and partner with families honestly. Each piece reinforces the others. Done right, special needs support stops being a burden you manage and starts being something families specifically seek you out for.
Ready to elevate your childcare management?
Join hundreds of childcare providers using Totsyly to save time, improve communication, and grow their centers.